Corneal and Anterior Segment Surgery
Diseases of the Cornea and Anterior Segment of the eye are increasing in prevalence. As we age, the incidence of age-related corneal degeneration increases, and corneal diseases are a significant cause of blindness in both developed, and developing countries. Fortunately, developments in surgical technique and ophthalmic technologies now allow us to successfully treat many blinding corneal conditions. Current forms of Corneal Transplantation, Artificial Cornea Surgery, Artificial Iris Surgery, and Pterygium Surgery can now be performed with less complications and good success rates.
The Cornea and Anterior Segment of the Eye
The cornea is the clear transparent window at the front of the eye, allowing light to focus and enter the eye. If the cornea is damaged or distorted by injuries or infection, or becomes cloudy due to various corneal diseases, vision may be significantly reduced, or lost. The cornea has several layers consisting of different tissue layers – some corneal diseases affect only inner or outer layers, while other corneal diseases may affect all the layers of the cornea. In addition to the cornea, other associated structures in the front, or anterior segment of the eye, such as the iris (pupil) or lens may also be affected. Abnormalities of the iris, such as iris defects or deficiencies, which may occur after trauma, glaucoma and after cataract surgery, adds further to visual deficiencies and glare. Technologies and surgical procedures now allow for replacement of the Cornea (Corneal Transplantation), and also the Iris (Artificial Iris Surgery), which can restore vision. This new approach of anterior segment reconstruction of the front of the eye combines the latest techniques of selective corneal replacement, iris, and lens replacement to restore vision in the most complex forms of damage to the front of the eye.
Corneal Transplantation
Corneal Transplantation is a surgical procedure, in which the diseased layers of the cornea are replaced by healthy donor corneal tissue donated by another individual when he or she passes away. The replacement of the cloudy cornea, with a clear and healthy new cornea, restores vision to the corneal transplant patient.
Current forms of Corneal Transplantation

The Cornea consists of several layers, and in many patients, not all the layers are diseased or damaged. In the past, corneal surgeons only performed one main procedure – the Penetrating Keratoplasty (PK) operation, whereby the entire central aspect of the cornea was replaced by a donor cornea – a full-thickness transplant. Today, we generally reserve PK procedures for the more severe cases of corneal blindness where the entire thickness of the cornea is opaque or abnormal, as full corneal replacement in a PK procedure in general has a higher risk of corneal transplant rejection and failure. In general, the risk of transplant rejection after PK is in the region of 10-15%.
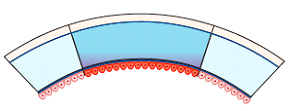
Diagram: Penetrating Keratoplasty – full-thickness replacement of the central cornea
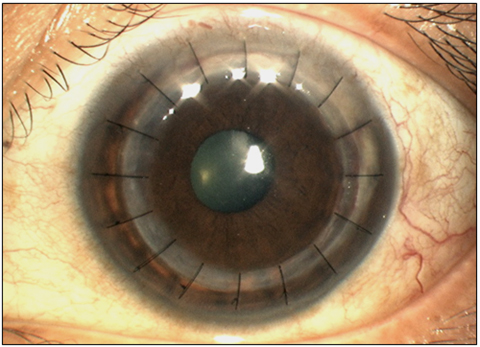 Penetrating Keratoplasty
Penetrating Keratoplasty
Several more recent forms of corneal transplantation procedures now exist, and it is now possible to selectively replace different layers of the cornea, whilst retaining the unaffected layers. The major advantages to just replacing the diseased layers, and leaving the healthy layers untouched, include a stronger eye after surgery, better visual quality, and most importantly, a marked reduction in complications during surgery, as well as after surgery, such as corneal transplant rejection, which leads to better long-term success rates overall. These forms of partial thickness corneal transplantation are termed Lamellar Keratoplasty procedures, and they have transformed how we perform corneal transplants today.
There are basically 2 forms of modern Lamellar Keratoplasty:
- Anterior Lamellar Keratoplasty (ALK)
ALK procedures involve exchanging only the front layers of the cornea, leaving the innermost layer (the Endothelial Layer), intact and unchanged. The commonest ALK procedure today is Deep Anterior Lamellar Keratoplasty (DALK), where all the front layers of the cornea are fully exchanged. The major advantage of DALK is that the risk of corneal transplant rejection is reduced to a 1-2% risk, compared to PK surgery, where the risk of rejection may be as high as 10-15%. With a well-performed DALK procedure, it is also often possible to achieve excellent visual quality, and because the risk of rejection is much less, less anti-rejection steroid eyedrops are used after surgery, which also means a reduction in other complications such as glaucoma, and infection. However, DALK in general is a more challenging surgical procedure compared to a PK procedure, the learning curve for DALK remains considerable.
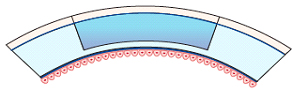
Diagram: Deep Anterior Lamellar Keratoplasty – Replacement of the front layers of cornea
 Deep Anterior Lamellar Keratoplasty
Deep Anterior Lamellar Keratoplasty
- Endothelial Keratoplasty (EK)
In many instances, corneal clouding is due to an ageing or abnormal innermost layer of the cornea, known as the Endothelial Layer, which consists of Endothelial Cells which are either insufficient in numbers or are damaged. EK procedures leave the front layers of the cornea intact, and instead just exchange the innermost layers which contain the endothelial cells needed to keep the cornea clear. Because the donor endothelial layer is usually inserted through as small side incision (similar to “keyhole surgery”), there are no sutures on the cornea (“sutureless surgery), and vision recovers much at an earlier rate than PK or ALK. EK is usually performed as a Day Surgery procedure, and can also be performed under Local Anesthesia (LA)(just an anesthetic injection around the eye), as opposed to a full General Anesthesia (GA). The risk of transplant rejection is also much lower than PK, and ranges from 1-8%.
There are 2 forms of EK surgery today, DSAEK (Descemets Stripping Automated Endothelial Keratoplasty), and DMEK (Descemets Membrane Endothelial Keratoplasty).
In DSAEK, a slightly thicker layer of inner corneal tissue, consisting of several layers, is transplanted – this procedure has been shown to have good vision restoration, less complications – rejection as compared to PK, in the region of 5-8%, and is therefore a relatively common form of transplantation in the West and in advanced countries.
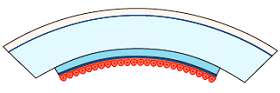
Diagram: Descemets Stripping Automated Endothelial Keratoplasty – Adding a new thin inner layer including the Endothelial Cell Layer
 Descemets Stripping Automated Endothelial Keratoplasty
Descemets Stripping Automated Endothelial Keratoplasty
DMEK is the most recent version of EK surgery, which improves on DSAEK surgery, in which only the innermost membrane and the endothelial cells are transplanted – this thin and delicate layer makes the surgery more challenging, and only a few surgeons perform this procedure at present, but the main advantages of DMEK is that the rejection rate is only about 1%, and DMEK offers the best quality after surgery.
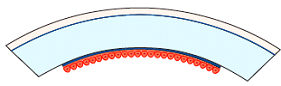
Diagram: Descemets Membrane Endothelial Keratoplasty – Just replacing the ultrathin Descemets Membrane Endothelial Cell Layer
 Descemets Membrane Endothelial Keratoplasty
Descemets Membrane Endothelial Keratoplasty
In both DSAEK and DMEK, repeat corneal transplantation can be more easily performed, as compared to PK surgery, and can also be combined with other forms of surgery such as cataract removal and intraocular lens implantation at the same sitting.
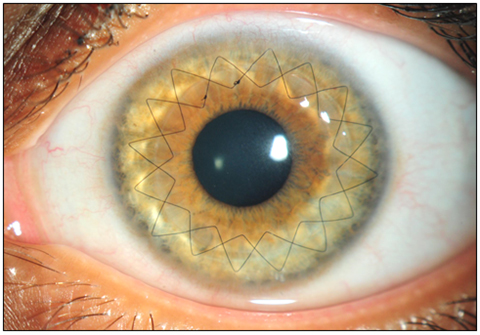
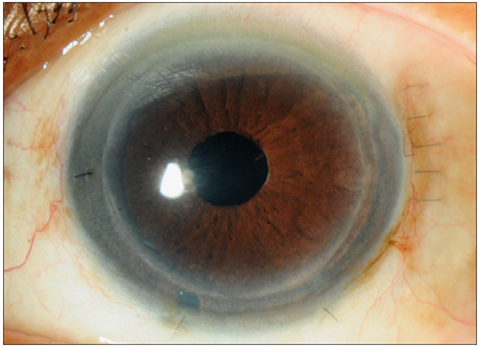
Artificial Iris Surgery
The iris is the brown (or blue) structure in the eye, which is behind the cornea, but in front of the lens, and has a central opening which is the pupil. In a normal iris, the size of the pupil can vary according to light exposure, constricting to reduce glare in bright light conditions, and dilating in dim light conditions, so as to improve vision and contrast. The iris may be inadvertently damaged by glaucoma, or during cataract surgery, and the pupil as a result no longer functions accordingly, and may be distorted or eccentric, which affects vision. In many cases of corneal transplantation, the iris can get stuck to the back of the corneal graft, which then leads to corneal damage and a much higher risk of corneal transplant rejection.
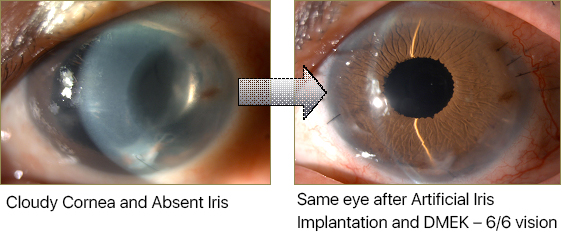
In recent years, an artificial iris has been developed, which has been shown to be effective, and safe, in replacing a damaged iris. The CustomFlex Artificial Iris from Humanoptics, is a US FDA-approved clinical device, and we have now begun to use this Artificial Iris to replace an absent, damaged pupil or iris, along with performing corneal transplantation, in a 2 stage procedure, so as to restore the full anatomy of the front of the eye. With an Artificial Iris in position, it is now possible to perform DMEK surgery in the most complex cases, where surgery would not have been possible, and removing the risk of iris tissue damaging the corneal cells, will reduce the risk of transplant rejection and enhance long term corneal transplant survival.
Artificial Cornea Surgery

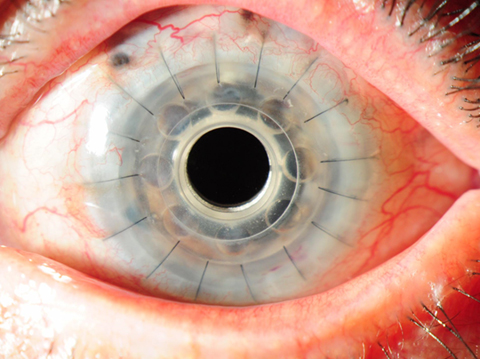 Boston Type 1 Keratoprosthesis
Boston Type 1 Keratoprosthesis
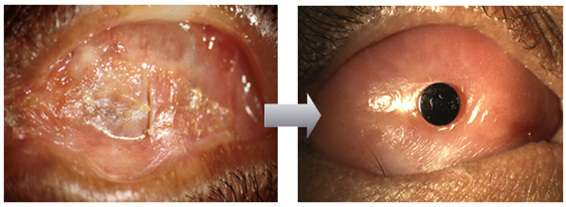 Osteo-Odonto Keratoprosthesis (OOKP)
Osteo-Odonto Keratoprosthesis (OOKP)